START SAVING WITH your GEMTESA Simple Savings Card!
GEMTESA® SIMPLE
SAVINGS PROGRAM

Member ID:
Group #: TCPGEM1
BIN #: 026241
PCN #: CRX
You may pay
As little as

For your
first prescription*
After your first prescription, continue to save on refills



*See full program terms, conditions, and eligibility criteria below.
PROGRAM TERMS, CONDITIONS, AND ELIGIBILITY CRITERIA
- This offer is valid only for eligible patients and is good for use only with a valid prescription for GEMTESA at
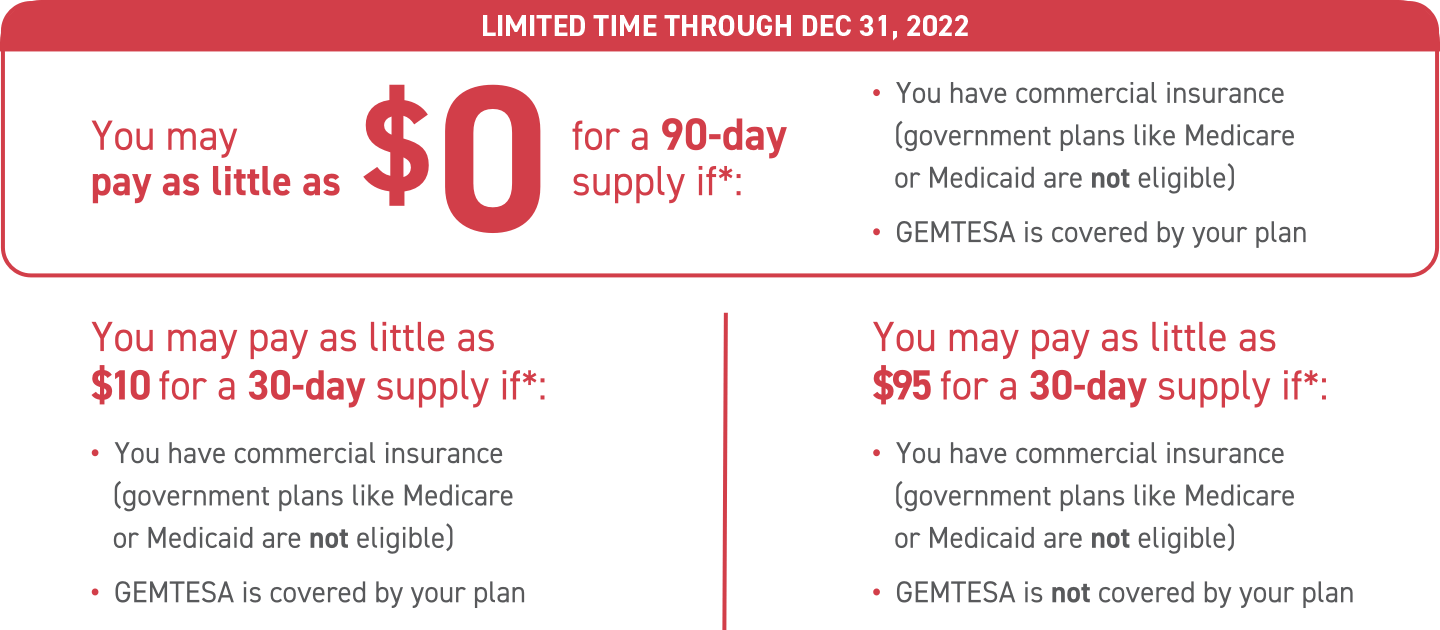
the time the prescription is filled by the pharmacist and dispensed to the patient. - Depending on your insurance coverage, most commercial patients for whom GEMTESA is covered pay as little
as $10 for a 30-day supply or could pay as little as $0 for a 90-day supply between October 1, 2021 and
December 31, 2022. Most commercial patients for whom GEMTESA is not covered pay as little as $95 for a 30-day
supply. Maximum savings limits apply; patient out-of-pocket expense will vary. - This card is valid for up to 12 prescription fills for a 30-day supply or 4 prescription fills for a 90-day supply.
- This card expires one-year from activation date.
- This offer is not valid for use by patients enrolled in Medicare, Medicaid, or other federal or state programs
(including any state pharmaceutical assistance programs), or private indemnity or HMO Insurance plans that
reimburse the patient for the entire cost of the prescription drugs. Patients may not use this offer if they are
Medicare-eligible and enrolled in an employer-sponsored health plan or prescription drug benefit program for
retirees. This offer is not valid for cash-paying patients. - Urovant Sciences reserves the right to rescind, revoke, or amend this offer without notice.
- Offer good only in the USA, including Puerto Rico, at participating retail pharmacies.
- Void where prohibited by law, taxed, or restricted.
- This card is not transferable. The selling, purchasing, trading, or counterfeiting of this card is
prohibited by law. - This card has no cash value and may not be used in combination with any other discount, coupon,
rebate, free trial, or similar offer for the specified prescription. - This offer is not health insurance.
- By redeeming this card, you acknowledge that you are an eligible patient and that you understand
and agree to comply with the terms and conditions of this offer.
For questions about this program please call 1-833-UROVANT (876-8268).
Pharmacist Instructions for a patient with an eligible third-party payer: When you redeem this card, you
certify that you have not submitted and will not submit a claim for reimbursement under any federal,
state, or other government health insurance programs for this prescription.
- Submit the claim to the primary third-party payer first and then submit the balance due as a Secondary Payer COB [coordination of benefits] with patient responsibility amount and a valid Other Coverage Code, (e.g. 3 or 8). The patient’s out-of-pocket expense will be reduced up to the maximum savings limit for the program.
- Valid Other Coverage Code required. For any questions regarding online processing, please call the Help Desk at 1-800-433-4893.